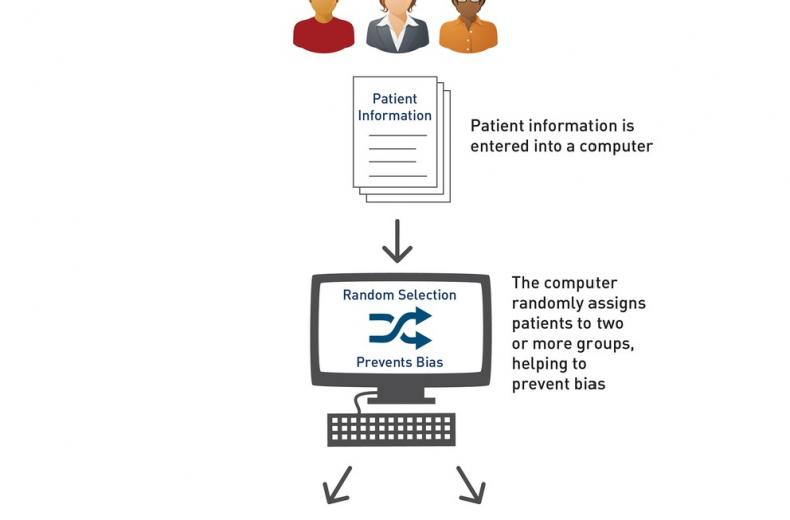






Randomization in clinical trials has been used since 1929 when R.A. Fisher implemented the first randomization scheme i.e. “the flip of a coin” in a tuberculosis trial. Randomization offers the POSSIBILITY of preventing selection bias that occurs due to the predictability of alternation. It is a method of experimental control. In randomized studies, it is required to generate randomization schedules which should be reproducible and contains random numbers for each patient.
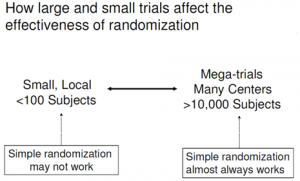
Simple randomization (i.e. flipping a coin) was the only method in place for many years but then researchers noticed that for certain situations, this was not ideal. There are several types of randomization techniques available in literature now. The most elementary method of randomization is unrestricted (simple) randomization in which treatments are allocated to patients in sequence based on a random number without any restriction.
 Although unrestricted randomization is an acceptable approach, however, block randomization technique has an advantage over it. Block randomization is also known as restricted randomization. Block randomization increases the comparability of the treatment groups, especially when patient characteristics may change over time, such as recruitment policy. Another benefit of block randomization is that the treatment groups are nearly of equal size. In crossover trials, it provides the means of obtaining balanced designs with their greater efficiency and easier interpretation. It is suggested to choose block lengths carefully that are sufficiently short to limit possible imbalance, but that is long enough to avoid predictability towards the end of the sequence in a block.
Although unrestricted randomization is an acceptable approach, however, block randomization technique has an advantage over it. Block randomization is also known as restricted randomization. Block randomization increases the comparability of the treatment groups, especially when patient characteristics may change over time, such as recruitment policy. Another benefit of block randomization is that the treatment groups are nearly of equal size. In crossover trials, it provides the means of obtaining balanced designs with their greater efficiency and easier interpretation. It is suggested to choose block lengths carefully that are sufficiently short to limit possible imbalance, but that is long enough to avoid predictability towards the end of the sequence in a block.
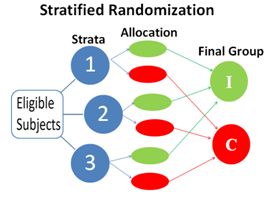 Stratified randomization is used when study population is heterogeneous in nature and one or a few baseline characteristics are strongly related to the outcome. It works well with small trials by preventing imbalance on major predictors but at risk of this data within strata. Stratified randomization is better over stratified analysis.
Stratified randomization is used when study population is heterogeneous in nature and one or a few baseline characteristics are strongly related to the outcome. It works well with small trials by preventing imbalance on major predictors but at risk of this data within strata. Stratified randomization is better over stratified analysis.
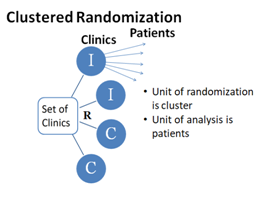 Cluster randomization is used when a group of individuals has to randomize instead of individuals. This technique has diminishing returns in precision and power as cluster size increases.
Cluster randomization is used when a group of individuals has to randomize instead of individuals. This technique has diminishing returns in precision and power as cluster size increases.
An adaptive randomization technique is a good example which uses prior information in a clinical trial design. The goal of an adaptive randomization is to maintain the integrity and validity of the study while giving the researcher flexibility in identifying the optimal treatment. It is possible only if outcome comes quickly and that is why pharmaceutical trials are commonly using adaptive randomization nowadays.
With randomization, masking is a very important aspect of blinding studies. Randomization will be successful only if masking is done properly.
In summary, it is suggested to use randomization technique carefully and maintain the integrity of the word “RANDOMIZATION” if used in the study. Also, the following statement must be avoided in method section:
- Randomization was done using computer-generated sequence.
- Randomization was stratified according to the hospital and tumour site (esophagus or cardia). No blocking was used within each of the four strata.
Randomization was done centrally by the coordinating centre. Randomisation followed computer-generated random sequences of digits that were different for each centre and for each sex, to achieve centre and sex stratification. Blocking was not used.
Disclaimer: The picture used in this blog is for education purpose only with no commercial usage.
Last modified: 21/11/2019