





Background
A 63-year-old female presented with complaints of abdominal pain with bloating for 7 days. She had fever for 5 days for which she was evaluated outside. CECT Whole Abdomen showed a large complex cystic lesion in the abdomen in the midline extending almost up to the level of umbilicus. It measured ~ 15 x 13 x 10cm. Mild free fluid in pelvis was seen. Serum CA-125 was 170U/ml. She underwent Total abdominal hysterectomy with bilateral salpingo-oopherectomy.
Gross Image

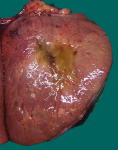
Fig.14a; Right ovarian cut surface- gross
On gross examination of right ovary reveals intact capsule with no surface involvement. Cut surface shows solid – cystic, firm areas with grey-white, glistening surface [Fig.14a]. Sections from ovary taken.
Microscopy

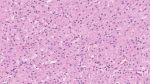
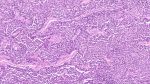
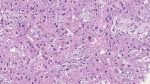
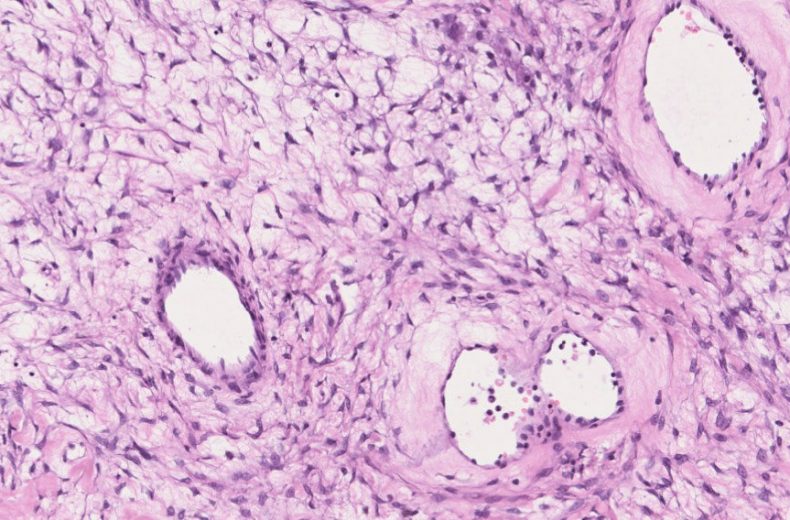
Fig.14b; H&E; 5x
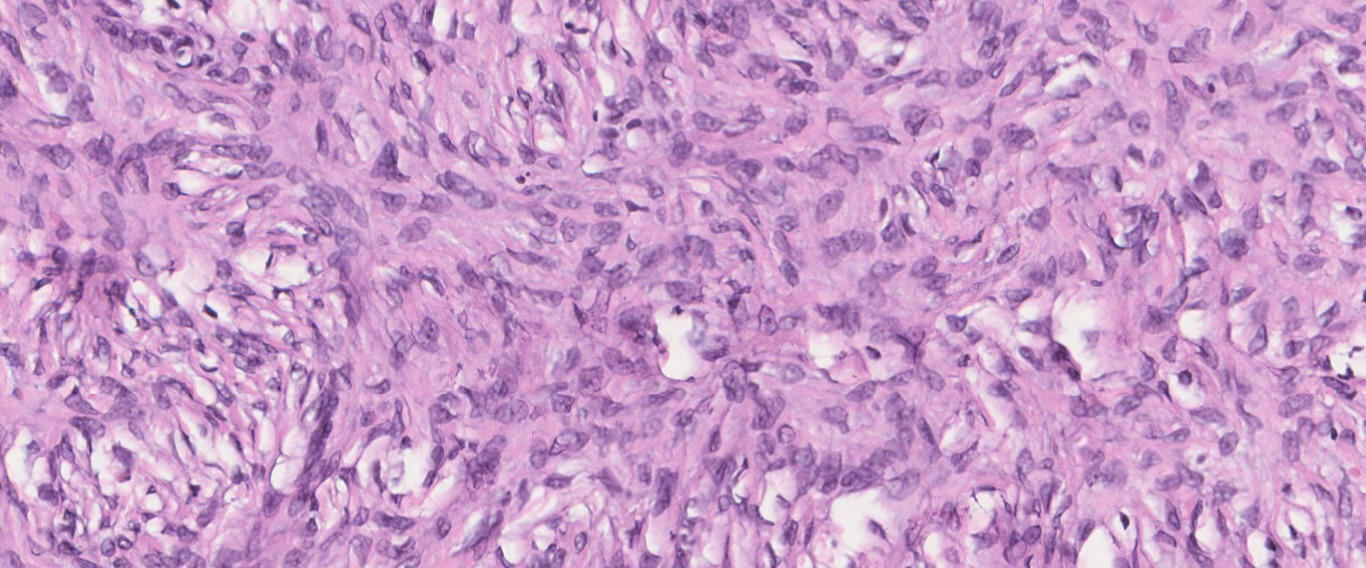
Fig.14c; H&E; 40x
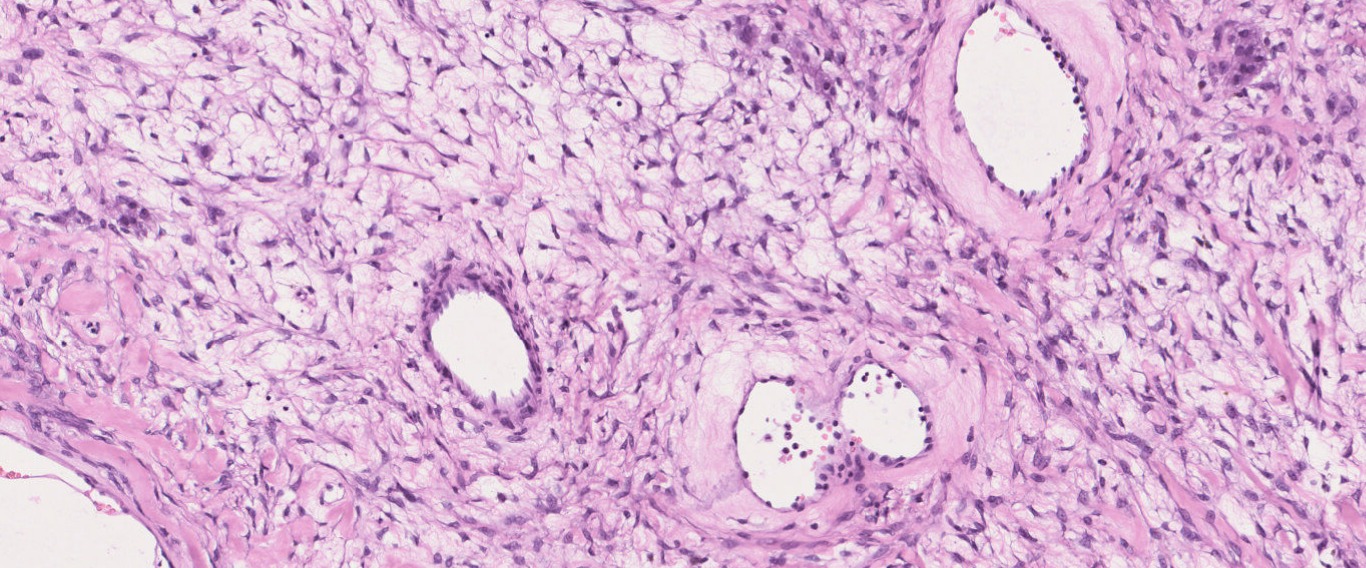
Fig.14d; H&E; 10x

Fig.14e; H&E; 20x

Fig.14f; H&E; 10x
Immunohistochemistry
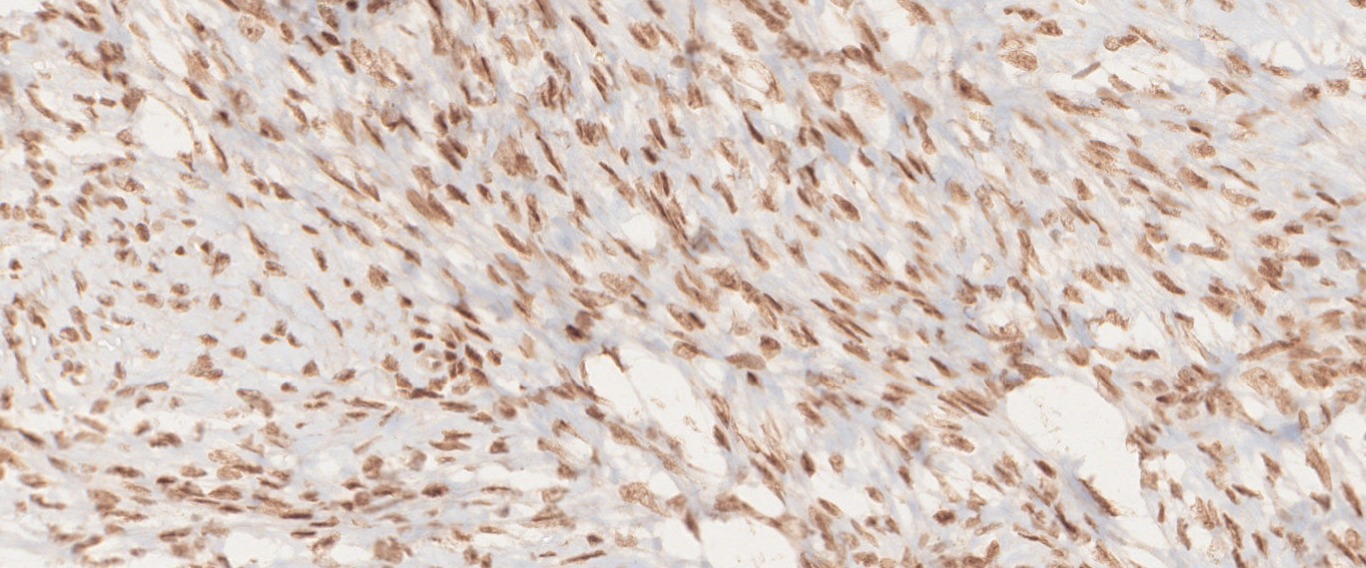
Fig.14g; SF-1

Fig.14h; SMA

Fig.14i; h-caldesmon
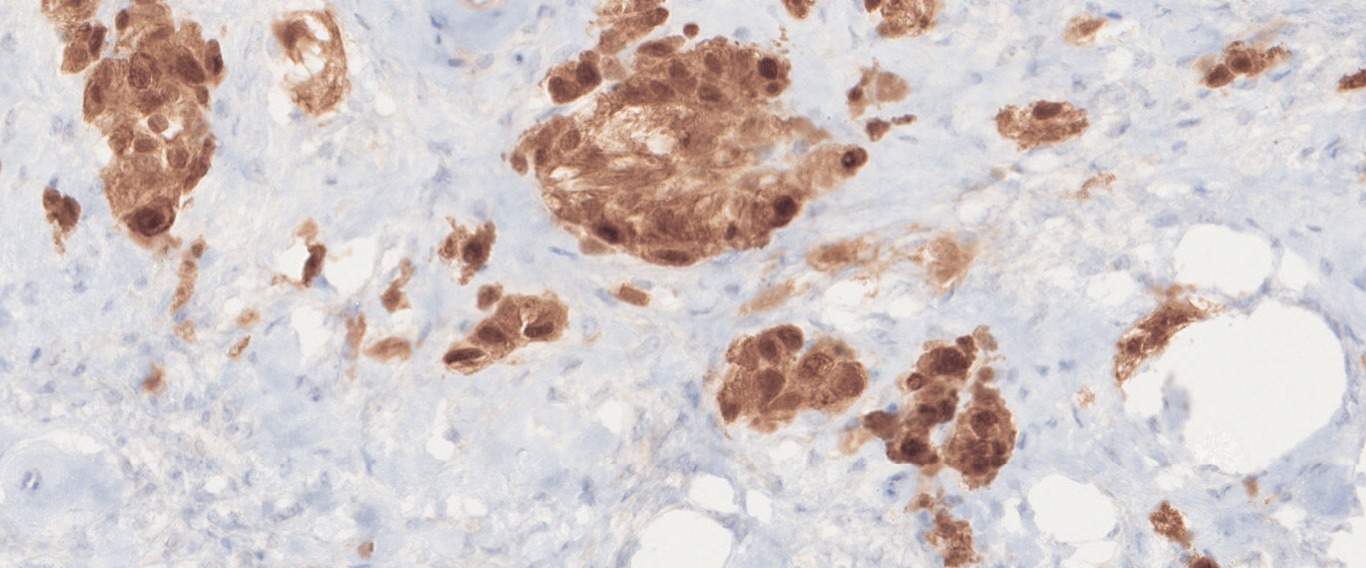
Fig.14j; Calretinin
Questions & Answers:
- What is your diagnosis?
- Which syndromes are associated with this tumor?
- Incidence: Fibrothecomas of ovary constitute about 4% of all ovarian tumors.
- Definition:
- They represent a group of benign tumors arising in stroma and exhibit a morphological spectrum consisting of entirely fibroblasts and producing collagen (Fibromas) to those containing plumper spindle cells with lipid droplets (Thecomas). When a tumor contains mixture of these cells, they are termed as fibrothecomas.
- Age of Presentation: all ages, more frequent during middle age.
- They are unilateral in about 90% cases and are rarely malignant.
- Clinical presentation: may be nonspecific such as pelvic and abdominal pain or distension. It may be accompanied by
- Meigs syndrome (ovarian fibroma, hydrothorax and ascites) OR
- Basal cell nevus syndrome (bilateral ovarian fibroma, multiple basal cell carcinoma of skin, odontogenic keratocysts, etc.
- Grossly, fibrothecomas are usually round, oval or lobulated encapsulated hard gray white masses covered by intact ovarian serosa.
- Edema and cystic degeneration are relatively common.
- Tumors >10cm tend to be associated with myxoid change or degeneration.
- Microscopically, the tumors are densely cellular, and the spindle-shaped cells have ill-defined cytoplasmic borders, round to oval hyperchromatic nuclei, and are arranged in patterns similar to those of typical fibromas.
- Fibromas are variably cellular, but in 10% of cases, the markedly increased cellularity warrants the diagnosis of cellular fibromas.
- Nuclei can be mildly or moderately atypical and between one and three mitotic figures per 10 HPF are usually present.
- These tumors can show myxoid change and degeneration.
- The term mitotically active cellular fibroma is recommended for any cellular fibroma with more than 4 mitoses per 10 HPF. In this setting, the absence of severe cellular atypia and abnormal mitotic figures should assist in the exclusion of fibrosarcoma.
- Ancillary studies: The use of ancillary techniques to distinguish between fibromas and thecomas is limited.
- Both tumors can be variably immunopositive for calretinin, alpha-inhibin, vimentin, SMA, WT-1, SF-1, ER, and PR .
- Intracellular lipid can also be identified in both types of tumors, although it is more diffuse in thecomas and only focal in fibromas.
- Genetic basis:
- In fibromas,trisomy and/or tetrasomy 12 is often found, and rarely IDH1 mutation.
- In cellular fibromas, loss of heterozygosity at 9q22.3 (PTCH1) and 19p13.3 (STK11) is frequent.
- FOXL2 mutations are absent which can be seen in occasional cases of thecomas.
- Early diagnosis and surgical resection are the treatment of choice for ovarian fibrothecomas and is associated with a good prognosis. Recurrences are common in cases of cellular fibromas and incomplete resections.
Contributed & Compiled by: Dr Nivedita Patnaik
In case of queries, email us at: patnaik.nivedita@rgcirc.org
Female genital tract Fibrothecoma Meigs syndrome Neoplasms Ovary Sex-cord stromal tumor
Last modified: 26/07/2021